Nationwide, employers provide coverage for most Americans under age 65, about 181 million people. And hospital care accounts for 44 cents of every personal health care dollar spent on those with private insurance.
The RAND study shows “market forces are clearly not working,” said Richard Scheffler, a health economist at the University of California, Berkeley. “Prices vary widely and are two and a half times higher than Medicare payment rates without any apparent reason,” he said.
The RAND researchers gathered information on 1,598 hospitals, about a third of the total number in the United States, using 4 million insurance claims from 2015 through 2017, a fraction of the total filed nationwide. The information was collected from employers, some insurers and state agencies. The study did not identify the employers, but researchers named individual hospitals through the information they obtained, a rare public listing.
The claims included a variety of services, ranging from a hospital stay for heart surgery to an outpatient visit to the emergency room. The researchers compared the claim as it would have been reimbursed by Medicare and what the private insurer paid to determine the overall difference in prices. The hospitals did not see the study before it was released.
The Indiana system, Parkview, says it is adopting new kinds of contracts. “At Parkview Health, we think the most important conversation is around what we can do moving forward, in strategic alignment with employers and insurance companies, to provide the highest quality care at the best cost,” said the company’s chief executive, Mike Packnett, in a statement.
Colorado Plains Medical Center did not respond to requests for comment.
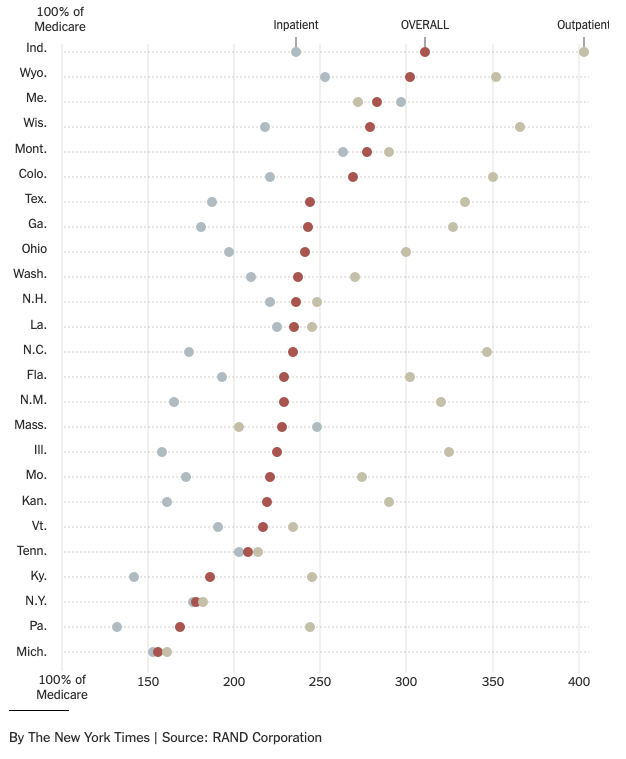
In New York and Pennsylvania, private prices were less than two times the Medicare rates. Indiana, which has the highest private prices among the 25 states analyzed, pays roughly three times what Medicare does.
Many businesses that contract with insurance companies have no idea what their insurers are paying individual hospitals in their plan’s network. “We’ve never seen what was agreed upon,” said Jennifer Fairman, the benefits manager for people who work for Larimer County in Colorado. “We’ve been signing these blank checks.”
But soaring hospital costs have become a significant burden, and many businesses have off-loaded more of the expense onto their employees through higher premiums and deductibles. Families have struggled to cope with surprise medical bills and increasing out-of-pocket costs. The trend toward consolidation in the last several years has also spurred higher costs, as hospitals merged into bigger, more powerful systems that dominated their local markets, demanding ever-higher prices.
Unlike Medicare, which sets the price it will pay for a type of care, insurers often try to negotiate discounts with hospitals over charges, especially for outpatient services, said Chapin White, an adjunct senior policy researcher at RAND and one of the authors of the study.
The insurers don’t have a strong incentive to demand the lowest prices because many, working for employers that are self-insured, are “literally spending someone else’s money,” he said. Insurers are also frequently paid based on how much the employer spends; they take in more revenue when the employer spends more.
Insurers say they are motivated to keep hospital prices low and point to the battles they sometimes have over whether a high-priced system will be in their networks.
One outlier was Michigan, where private prices run about 1.5 times Medicare rates. The auto industry and unions that represent autoworkers have put pressure on the major Blue Cross plan to hold hospital prices down. “To keep the market in check, you need a plan to throw its weight around and employers to back them up,” Mr. White said.
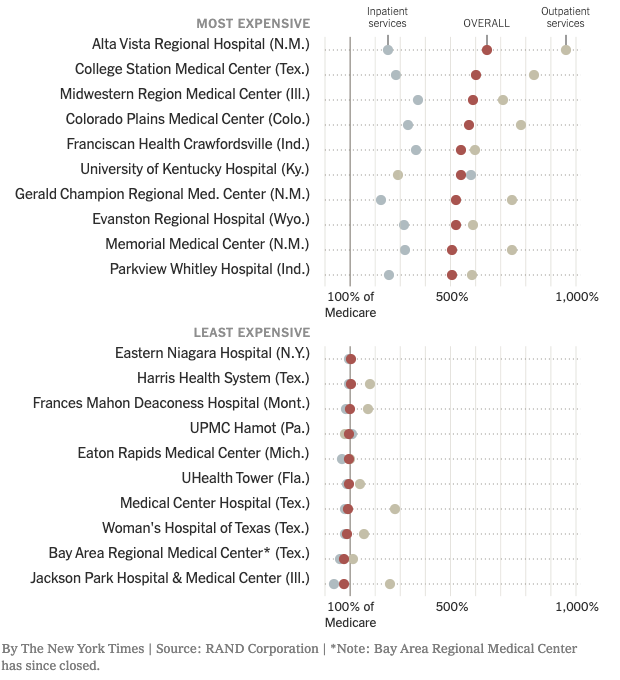
Individual Hospitals
The study’s most and least expensive hospitals for private insurers, compared with what Medicare would pay.